Select your language
")
")

Knee Anatomy
The knee joint is one of the largest and one of the most complex joints in the human body.To achieve the result of the knee's multiform movement requires the strict and detailed cooperation of many anatomical molecules that make up this joint. Due to its complex anatomical structure, it is extremely prone not only to injury, but also to damage.
The ligamentous structures define the limits of movement of the joint while the musculotendinous units control the movement of the joint.
The knee joint consists of four main bones, the femur, the tibia, the fibula and a small flat bone on the front surface of the joint, the patella. These bones form two joints between them the tibiofemoral(where the two femoral condyles come into contact with the tibial tubercles), and the patellofemoral (where the patella comes into contact with the femur).The ends of the bones are covered by articular cartilage, and the tissue that connects them surrounding the joint is called the articular capsule. Between the bones are the menisci and the 2 cruciate ligaments (anterior and posterior cruciate ligaments ).The stability of the knee is enhanced by the ligaments and the muscles surrounding it. Static stability is provided by the ligaments , the bursa , the menisci and the bones; dynamic stability is provided by the muscles surrounding the joint.
The main anatomical structures of the knee joint are:
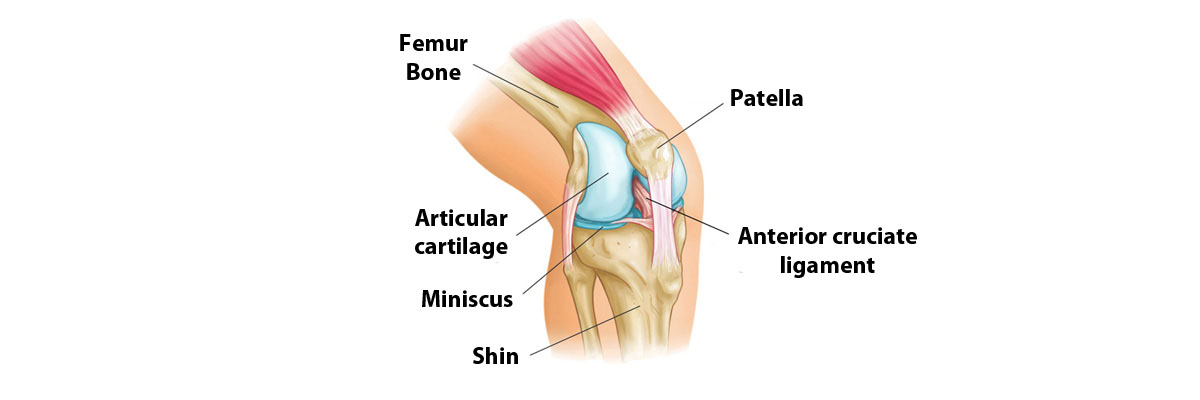
Meniscus
The menisci are two menoid-shaped fibrocartilaginous structures.The inner meniscus is C-shaped while the outer meniscus is more circular.They are inserted between the articulated bones like cushions and their role is to dampen the applied pressures and absorb shocks.
Basic functions of the Meniscus
1) They transfer loads from the thigh to the shin.
2) They contribute significantly to the stability of the joint, especially the posterior horn of the medial meniscus.
3) They convert the sliding movement into a friction movement since movement of both of these forms takes place at the knee
4) Smooth the discrepancy in the shape of the articular surfaces of the femoral and tibial tubercles
5) They increase the contact surface by interposing between two uneven surfaces absorbing the vibrations of the knee (like a kind of shock absorber).
6) They help to lubricate the joint with synovial fluid, contributing to its distribution within the joint cavity of the knee.
There are four ligaments that connect the femur to the tibia, 2 cruciate ligaments (anterior and posterior) and 2 lateral ligaments (medial and lateral).
The anterior and posterior cruciate ligaments are used to stabilize the knee at its center.They are called cruciates because they interlock as they attach to the tibia and femur.
The anterior cruciate ligament, located in the centre of the knee, limits the rotation, but also the forward movement of the tibia.
The posterior cruciate ligament, also located in the centre of the knee joint, limiting the backward movement of the tibia.
Side Connectors
There are two lateral links. They are located one on each side of the knee. The medial and lateral collateral ligaments arise from the supraspinous processes of the femoral condyles and take refuge, the lateral collateral ligament in the head of the fibula and the medial collateral ligament in the medial surface of the tibia. Their role is decisive as they control the lateral stability of the knee joint. In injuries of the collateral ligaments, the knee opens on the medial or lateral side depending on the extent of the damage. It is possible for the knee's collateral ligaments to be torn, partially torn or totally torn.
The knee joint is the largest joint in the body, between the thigh bone and the tibia-femur.
The articular cartilage that covers the articular surface is a common cause of knee pain because it is a tissue that has no vascularity, so any damage or wear is not easily healed.
The sooner a cartilage problem is diagnosed, the better the treatment results will be.
Other structures in the knee joint that are often injured are the menisci (inside and outside), ligaments and tendons.
In fact, often injuries involve more than one of these structures.
The conditions affect a large percentage of the population without age differentiation and can be either degenerative (e.g. osteoarthritis) or traumatic (e.g. ruptures of the meniscus, cruciate ligaments, patellar dislocation.
Symptoms include pain that may limit daily activities, a feeling of weakness or instability, difficulty bending or extending the leg, swelling or swelling.
In addition to conservative, drug or minimally invasive injectable treatments, many of the conditions require arthroscopic or surgical treatment.